|
Experimental
VII. Other cardiac assist
devices
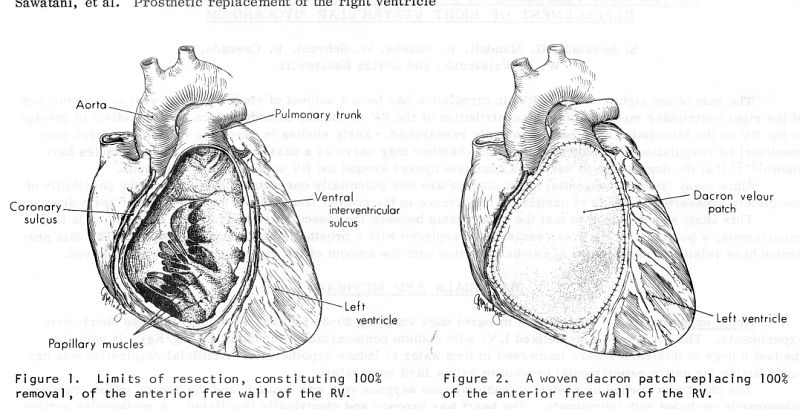
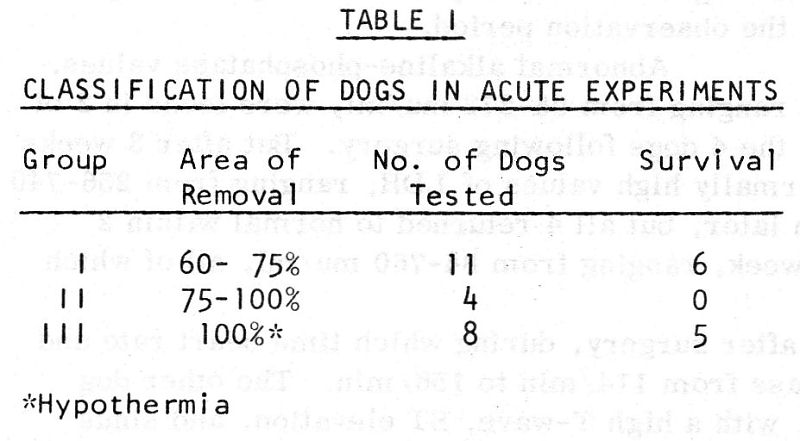
A. Prosthetic replacement of the
right ventricular wall (1974)
Summary
The role of
the right ventricle (RV) in circulation, the function of the right
ventricular myocardium, the contribution of the RV to normal
hemodynamics, and the effects of damage to the RV on the circulation
have been studied previously. This study was designed to test the
relationship between the musculature and function of the RV. Since
many types of congenital heart disease are now potentially correctable
by surgery, the possibility of completely bypassing the RV is of
particular importance. In our experiments, various portions the RV
were excised and replaced with a prosthetic patch made of dacron and
hemodynamic data were collected.
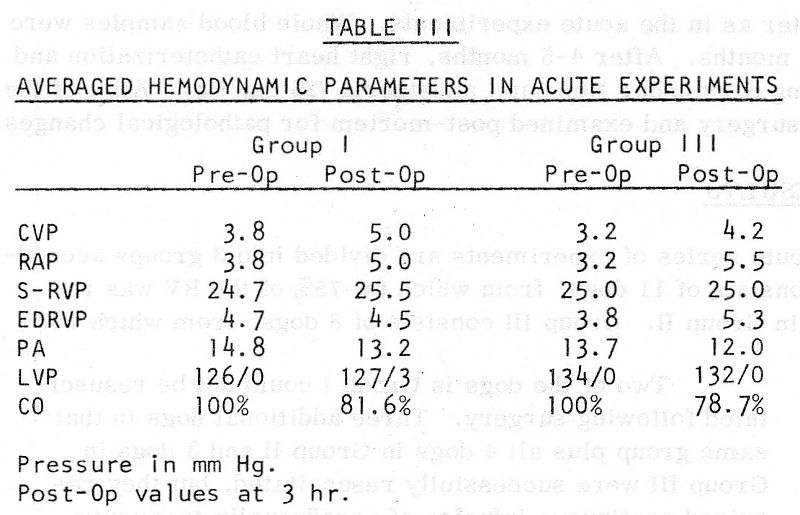
In acute
experiments, 23 dogs were divided in 3
groups according to the amount of the resected RV free wall. Their
survival (11/23 dogs successfully resuscitated from surgery) and data
collected 3 hours after completion of surgery in these surviving dogs
are shown below. There were only mild hemodynamic changes in the
surviving dogs.
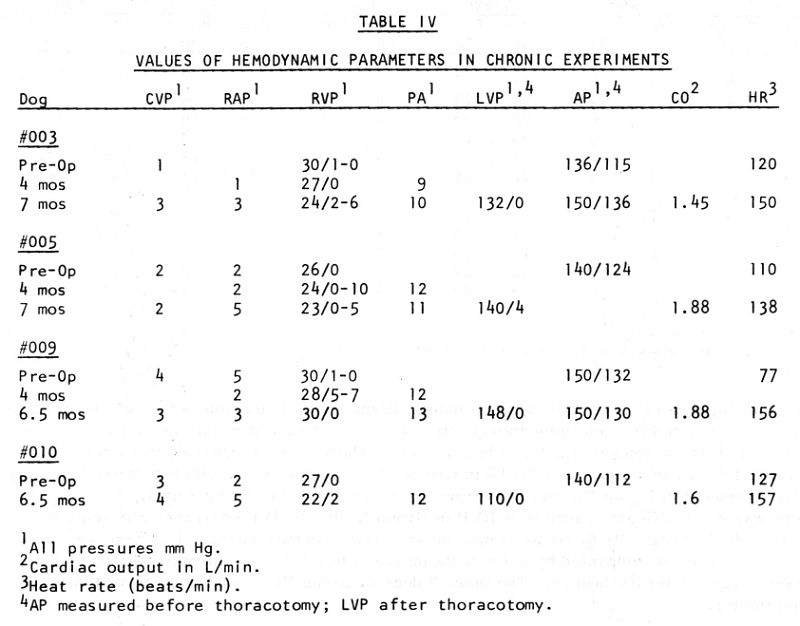
In chronic
experiments, 10 dogs were studied.
Approximately 75% of the wall of the RV was removed and replaced by
the patch, baseline data were recorded, dogs were allowed to recover.
Six dogs died within 17 days after surgery from
various causes. Hemodynamic data were again collected after approx. 4
and 7 months in the 4 surviving dogs. Their general health was good.
Their hemodynamic function was normal and differed little from
pre-operative hemodynamic values. The cineangiograms showed that the
RV contracted and emptied well and during systole, the septum moved
towards the RV space and the RV anterior wall moved toward the septum,
reducing the RV volume.
Pathologic
examination showed good healing along the suture line with smooth and
well-organized fibrous layer of pseudo-intima, including a
single-celled layer of endothelium over the blood/tissue surface
covering. The patch was uniformly wrinkled with reduced surface area
(to 35-45% as compared to 75% of the free wall at the time of
surgery). This was accompanied by elongation of the remaining wall of
the RV
The results
reported here indicate that in dogs the LV alone, in the absence of a
kinetic RV, is capable of maintaining normal hemodynamics (when the RV
free wall is replaced by a non-distensible and non-contractile dacron
patch.
Publication:
Ventricular performance following ablation and prosthetic
replacement of right ventricular myocardium.
Sawatani, S; Mandell, G; Kusaba, E; Schraut, W; Cascade, P;
Wajszczuk, W J; Kantrowitz, A. Trans Am Soc Artif Intern
Organs. 20 B: 629-36, 1974.
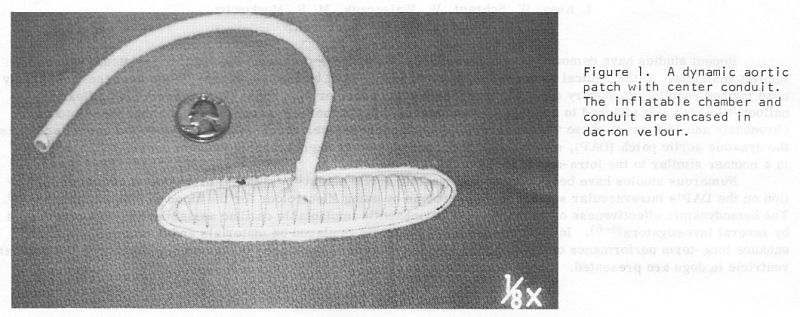
B. Dynamic Aortic patch – an
auxiliary ventricle (1974)
Summary
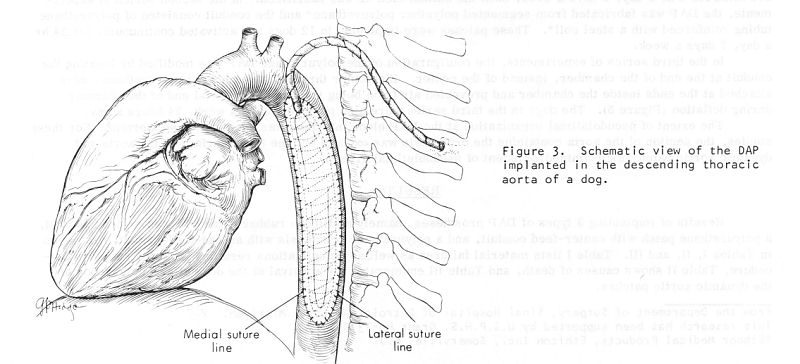
The Dynamic Aortic Patch (DAP)
is a permanent device, a prosthesis developed in this laboratory for
implantation in the descending aorta. It is activated in a manner
similar to the intra-aortic balloon. Initial problems with clot
formation on its blood contact surface have been overcome and its
hemodynamic effectiveness was established. In the present study
emphasis is placed on materials and configurations which enhance
long-term performance of the implant. Findings based on prolonged in
vivo performance with this auxiliary ventricle (DAP) in dogs are
presented. Different materials and configuration of the device and
pumping durations were tested.
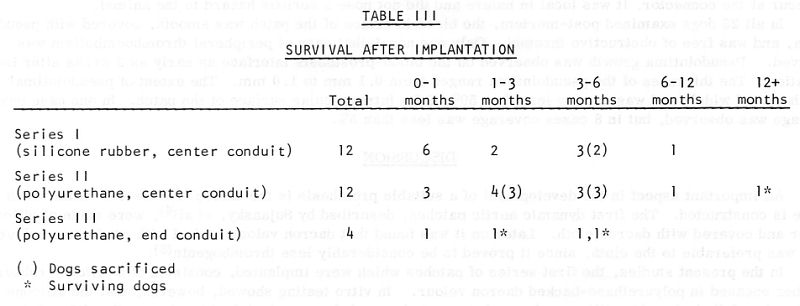
In the series of tests, using dynamic aortic patches with silicone
rubber chambers and conduits, no material failure occurred in vivo.
However, in vitro testing indicated that the flex life of the material
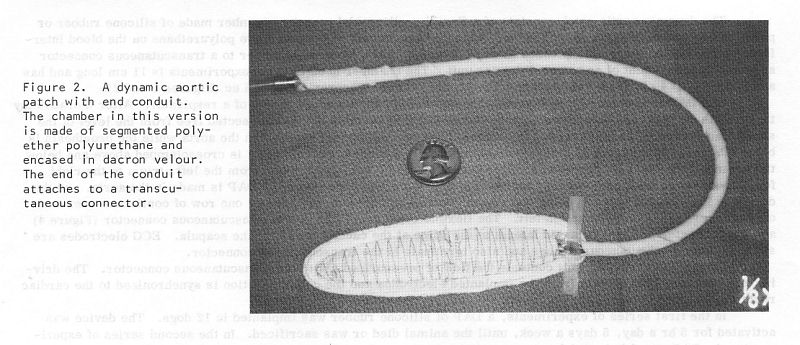
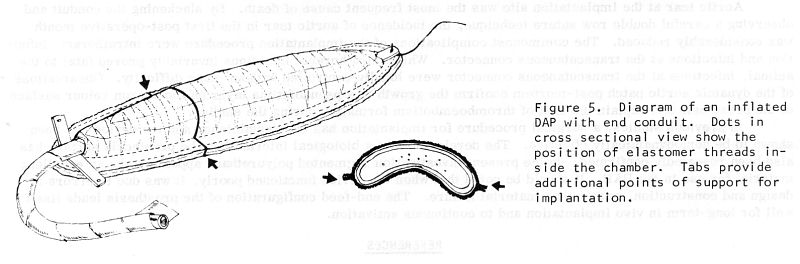
was limited to less than continuous use. Devices, with segmented
polyurethane pumping chambers and steel coil reinforced polyurethane
conduits, performed satisfactorily, particularly when the conduit was
attached at the end of the pumping chamber. One animal from the
second series, with the polyurethane implant activated for 16 months,
is alive and healthy. Aortic tear at the implantation site was the
most frequent cause of death. By slackening the conduit and
observing a careful double row suture technique, the incidence of
aortic tear in the first post-operative month was considerably
reduced.
The commonest complications of the implantation procedure were
intrathoracic infection and infections at the transcutaneous
connector. While intrathoracic infections invariably proved fatal to
the animal, infections at the transcutaneous connector were locally
controlled without much difficulty.
Observations of the dynamic aortic patch post-mortem confirm the
growth of a pseudointima layer on the dacron velour surface of the
prosthesis and explain the lack of thromboembolism formation during
the studies.
In the present investigation segmented polyurethane appears to be an
excellent material for use in the DAP. It should be noted that when
the device functioned poorly, it was due to errors in design and
construction, rather than material failure. The end-feed
configuration of the prosthesis lends itself well for long-term in
vivo implantation and to continuous activation.
Publication:
Long-term in vivo testing of an auxiliary
ventricle.
Kiso I,
Schraut W,
Wajszczuk W,
Moskowitz MS,
Freed P,
Kantrowitz A.
Transactions -
American Society for Artificial Internal Organs. 1974; 20 B:637-42.
C. Combined intra-aortic and
intra-ventricular pumping in cardiogenic shock – 1978
Summary
Combined intra-aortic and intraventricular counterpulsation for
treatment of experimental shock due to myocardial infarction, which
was induced in 5 dogs weighing 25-35 kg by ligation of the left
anterior coronary artery, is described. The technique is our own
original development in which a spherical balloon of only about 5 ml
capacity is used for intraventricular counterpulsation. The balloon is
fixed to the end of a conventional catheter and it can he introduced
into the left ventricle through the large vessels, avoiding thus the
necessity of performing a major operation on open chest. By
maintaining appropriate working conditions of the whole system
(delays, filling time, beginning of the time of collapse of both
balloons working in opposite phases: the intraventricular and the
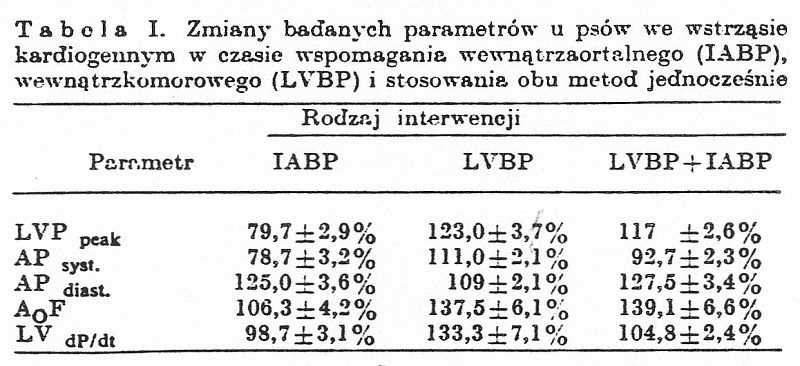
intra-aortic) it was possible to achieve a very favourable effect on
the haemodynamics, with a nearly 40°/o rise in the aortic blood flow,
increased aortic pressure by about 30% and only slight rise of the
dP/dt by about 5°/o.
Combined LVBP + IABP assistance results in a much more favourable
haemodynamic effect that intra-aortic counterpulsation or
intraventricular assistance alone, (which increases significantly
the requirements for oxygen). The size of the LV balloon should not
exceed 1/4-1/5 of the LV ejection fraction.
Publication:
SIMULTANEOUS INTRA-VENTRICULAR AND
INTRA-AORTIC COUNTERPULSATION IN TREATMENT OF EXPERIMENAL
CARDIOGENIC SHOCK. R. J. Zochowski, M.
J. Stopczyk, W. Wajszczuk. Kardiologia Polska, vol. 21,
No. 4, 349-357, 1978
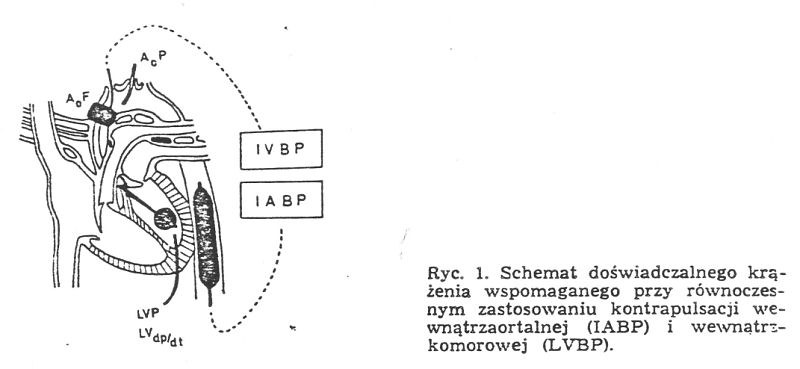
RYSZARD JACEK
2OCHOWSKI, MARIUSZ JAN STOPCZYK*, WALDEMAR WAJSZCZUK. Zastosowanie
równoczesnego wspomagania wewnątrzkomorowego i wewnątrzaortalnego do
leczenia eksperymentalnego wstrząsu kardiogennego.
Kardiologia Polska, XXI, Nr. 4, 349-357, 1978
Z Kliniki
Kardiologii Instytutu Chorób Wewnętrznych AM w Warszawie; kierownik:
doc. dr hab. n. med. T. Kraska i z Sinai Hospital
of Detroit and Wayne State University, Detroit, Michigan, USA
W pracy
przedstawiono metodę skojarzonego zastosowania kontrapulsacji
wewnątrzaortalnej i wspomagania wewnątrzkomorowego do leczenia
cksperymentalnego wstrząsu zawałowego.
Opisana technika
stanowi własne oryginalne rozwiązanie metodyczne, polegające na
zastosowaniu do wspomagania wewnątrzkomorowego kulistego balona o
pojemności tylko około 5 ml, który zamontowany na końcu
konwencjonalnego cewnika daje się wprowadzić do światła lewej komory
drogą przeznaczyniową, przez co pozwala uniknąć wykonywania dużego
zabiegu operacyjnego na otwartej klatce. Przy zachowaniu odpowiednich
warunków pracy obu systemów wspomagających (opóźnienia, czas
wypełniania i początek okresu zapadania obu pracujących w przeciwfazie
balonów: wewnątrzkomorowego i wewnątrzaortalnego) udało się osiągnąc
nadzwyczaj korzystny efekt hemodynamiczny, wyrażający się wzrostem
przepływu aortalnego o okolo 40%, rozkurczowego ciśnienia aortalnego o
około 30% przy nieznacznym tylko wzroście dP/dt o okolo 5%.
Skojarzone
wspomaganie LVBP + IABP daje w rezultacie znacznie korzystniejszy
efekt hemodynamiczny niż sama kontrapulsacja wewnątrzaortalna lub
zwiększające w sposób istotny zapotrzebowanie tlenowe wspomaganie
wewnątrzkomorowe.
WNIOSKI
1. Przedstawiony
model eksperymentalny spełnia w pełni warunki badania wpływu krążenia
wspomaganego na hemodynamikę wstrząsu kardiogennego.
2. Krążenie
wspomagane przy zastosowaniu dwóch pracujących w przeciwfazie balonów,
wewnątrzaortalnego i wewnątrzkomorowego przynosi korzystny efekt
hemodynamiczny, wyraźnie większy niż w przypadku stosowania jedynie
kontrapulsacji wewnątrzaortalnej (IABP) lub wewnątrzkomorowej (LVBP).
3. Zastosowanie do
wspomagania wewnątrzkomorowego balona nieprzekraczającego 1/4-1/5
objętości wyrzutowej lewej komory jest całkowicie wystarczające dla
osiągnięcia korzystnego efektu hemodynamicznego i czyni tą metodę
możliwą do zastosowania bez otwierania klatki piersiowej.
 |